In two multicenter, randomized, double-blind, placebo-controlled clinical trials:
Patients who received EGRIFTA® experienced:
Average reduction in EVAF*†
Main Phase
26 weeks
16%
Extension Phase
52 weeks
18%
In a post-hoc responder analysis*†‡ of data from two multicenter, randomized, double-blind, placebo-controlled clinical trials:
EGRIFTA® responders experienced:
Average reduction in EVAF*†
Main Phase
26 weeks
27%
Extension Phase
52 weeks
31%
Read on to explore the full efficacy outcomes and study designs of Studies 1 and 2 and their post-hoc analysis.
The results of the post-hoc analysis were not part of the NDA and therefore were not reviewed by the FDA to support the approval of EGRIFTA®.
The safety and effectiveness of EGRIFTA WRTM has been established based on adequate and well-controlled studies with EGRIFTA® (tesamorelin for injection).
EGRIFTA WRTM is not indicated for weight loss management.
EGRIFTA WRTM is not approved for use in clinical conditions other than the reduction of EVAF.
* The primary outcome for these trials was change from Week 0–26 in VAT by treatment group.
† A single-slice CT scan was used to quantify VAT.
‡ An ≥8% decrease in VAT area was determined to be clinically significant and used to define responders a priori.
EGRIFTA WRTM Summary Brochure
Learn about the EGRIFTA WRTM mechanism of action, key data, dosing and administration, and more.
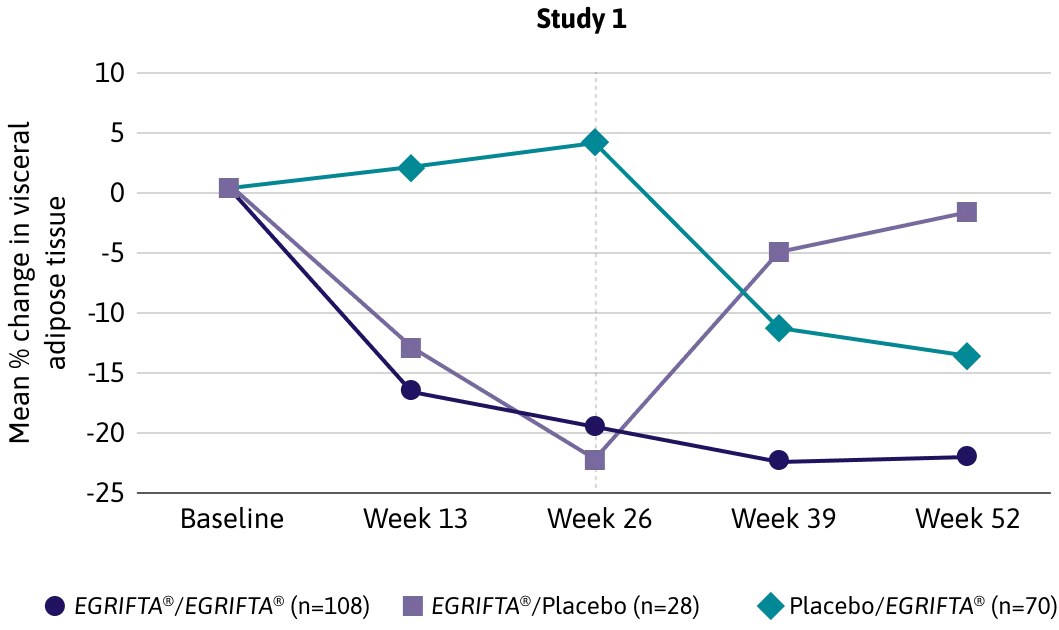
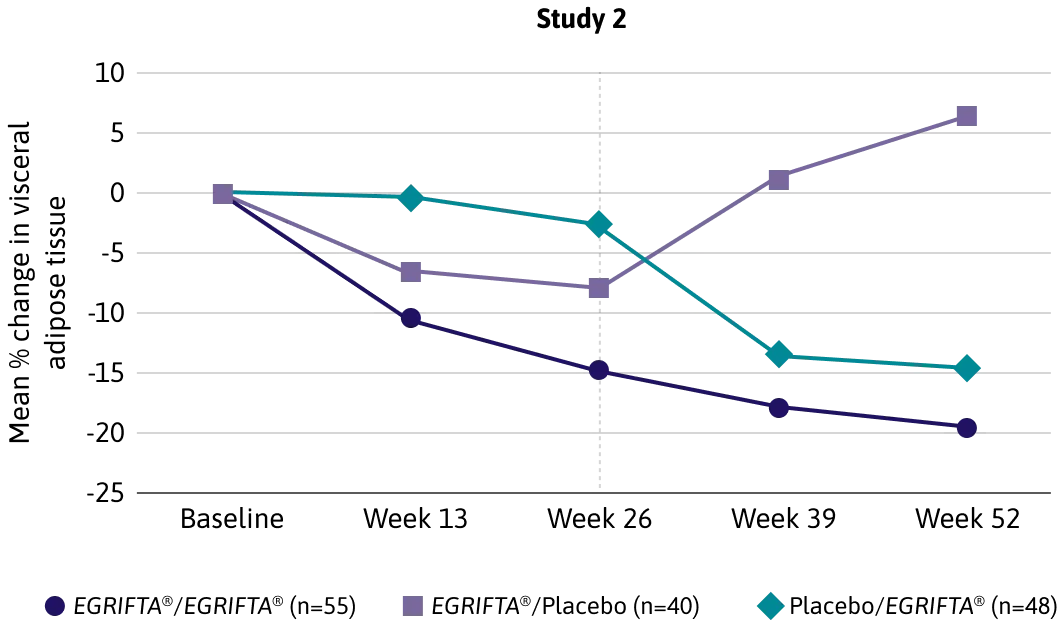
Studies 1 and 2: Pivotal Clinical Trials
In two multicenter, randomized, double-blind, placebo-controlled clinical trials:
Patients who received EGRIFTA® experienced a significant reduction in EVAF1*†
Average reduction in EVAF*†
Main Phase
26 weeks
16%
Extension Phase
52 weeks
18%
An expert panel in agreement with the FDA determined that a ≥8% decrease in EVAF was clinically significant.2
The safety and effectiveness of EGRIFTA WRTM has been established based on adequate and well-controlled studies with EGRIFTA® (tesamorelin for injection).1
EGRIFTA WRTM has a weight neutral effect and may increase lean body mass by up to 5 lbs.1,3
* The primary outcome for these trials was change from Week 0–26 in VAT by treatment group.
† A single-slice CT scan was used to quantify VAT.
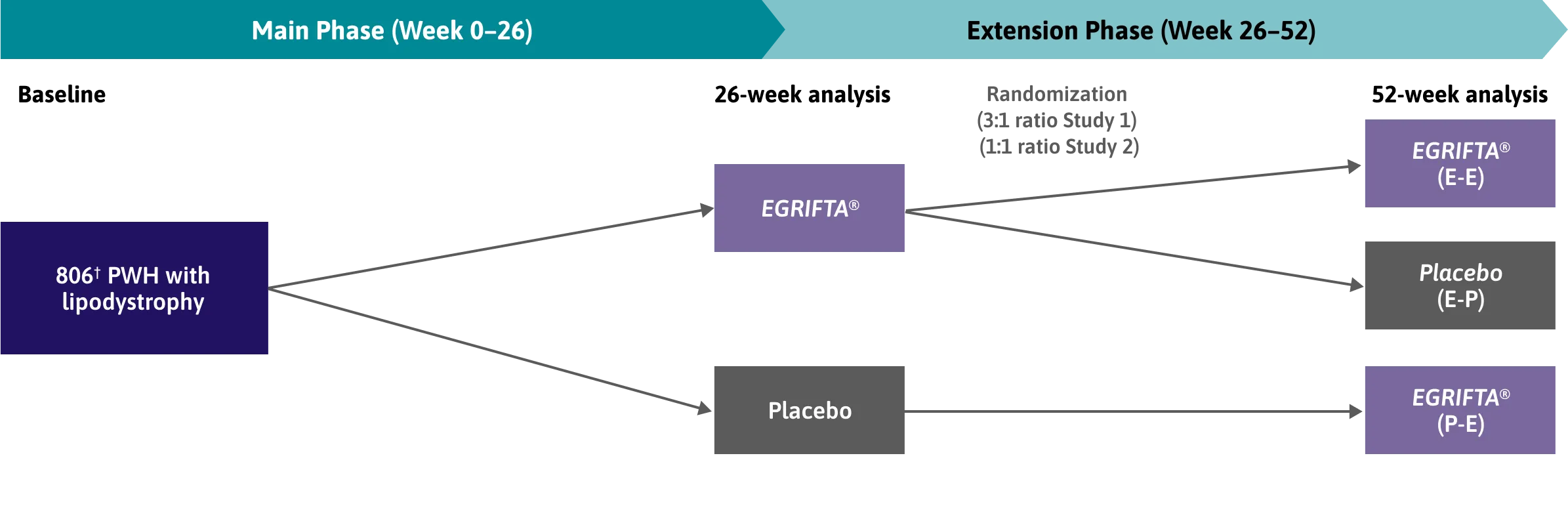
Main inclusion criteria1*
HIV-positive adults, 18-65 years old
EVAF accumulation
Stable ART for ≥8 weeks prior to baseline
In the Main Phase studies:1
543 patients received EGRIFTA®
263 patients received placebo
The safety and effectiveness of EGRIFTA WRTM has been established based on adequate and well-controlled studies with EGRIFTA® (tesamorelin for injection).1
E = EGRIFTA®. P = placebo. First letter refers to Main Phase, second letter refers to Extension Phase.
* Key exclusion criteria included FBG >150 mg/dL (>8.33 mmol/L), BMI ≤20 kg/m2, diabetes type 1 or insulin‑treated type 2, use of insulin‑sensitizing agent, or a history of malignancy or active neoplasm.
† 816 were included and underwent randomization, 806 received treatment as assigned.
Post-Hoc Responder Analysis*†
In a post-hoc responder analysis*† of data from two multicenter, randomized, double-blind, placebo-controlled clinical trials:
EGRIFTA® responders experienced a significant reduction in VAT at 26 weeks that was maintained for up to 52 weeks3*
Average reduction in EVAF*†
Main Phase
26 weeks
27%
Extension Phase
52 weeks
31%
Among responders, VAT:3‡
Decreased from 187 cm2 to 137 cm2, approaching normal levels (<130 cm2) by Week 26.
Was, on average, at normal levels (mean VAT: 129 ± 48 cm2) at Week 52.
The results of the post-hoc analysis were not part of the NDA and therefore were not reviewed by the FDA to support the approval of EGRIFTA®.
The safety and effectiveness of EGRIFTA WRTM has been established based on adequate and well-controlled studies with EGRIFTA® (tesamorelin for injection).
EGRIFTA WRTM is not indicated for weight loss management.
EGRIFTA WRTM is not approved for use in clinical conditions other than the reduction of EVAF.
* The primary outcome for these trials was change from Week 0–26 in VAT by treatment group.
† An ≥8% decrease in VAT area was determined to be clinically significant and used to define responders a priori.
‡ A single-slice CT scan was used to quantify VAT.
In a post-hoc responder analysis*† of data from two multicenter, randomized, double-blind, placebo-controlled clinical trials:
EGRIFTA® effects on secondary metabolic outcome measures in PWH, WC, lean body mass, and trunk fat3
Average reduction in waist circumference*†
Main Phase
26 weeks
1.65” (4.2 cm)
Extension Phase
52 weeks
1.85” (4.7 cm)
Secondary metabolic outcomes‡
Outcome
Change from Week 0–26 (n=232)
Change from Week 0–52 (n=110)
Baseline
Change
Baseline
Change
WC (cm)
103.7 ± 8.6
-4.2 ± 5.7§
103.6 ± 8.2
-4.7 ± 6.4**
Lean body mass (kg)
62.2 ± 9.6
1.6 ± 2.4§
62.1 ± 9.1
1.2 ± 2.8**
Trunk fat (kg)
14.4 ± 4.7
-1.8 ± 2.0§
14.4 ± 4.4
-2.2 ± 2.3**
The results of the post-hoc analysis were not part of the NDA and therefore were not reviewed by the FDA to support the approval of EGRIFTA®.
The safety and effectiveness of EGRIFTA WRTM has been established based on adequate and well-controlled studies with EGRIFTA® (tesamorelin for injection).
EGRIFTA WRTM is not indicated for weight loss management.
EGRIFTA WRTM is not approved for use in clinical conditions other than the reduction of EVAF.
* The primary outcome for these trials was change from Week 0–26 in VAT by treatment group.
† An ≥8% decrease in VAT area was determined to be clinically significant and used to define responders a priori.
‡ All data presented as mean ± SD, unless stated otherwise.
§ Indicates p<0.05 for within group-comparison of baseline vs. 26 weeks, using a mixed repeated measure model.
** Indicates p<0.05 for within group-comparison of baseline vs. 52 weeks, using a mixed repeated measure model.
EGRIFTA® responders demonstrated statistically significant differences in secondary metabolic outcomes compared to non-responders, including:1,3
Measures of glucose homeostasis
Other outcomes
Fasting glucose levels‡
Fasting insulin levels§
HbA1c levels¶
HOMA-IR score**
2-hour glucose levels††
Triglyceride levels‡‡
Adiponectin levels§§
Improvements in triglyceride and adiponectin levels, as well as the preservation of long-term glucose homeostasis suggest metabolic benefits associated with reducing VAT.3
The results of the post-hoc analysis were not part of the NDA and therefore were not reviewed by the FDA to support the approval of EGRIFTA®.
The safety and effectiveness of EGRIFTA WRTM has been established based on adequate and well-controlled studies with EGRIFTA® (tesamorelin for injection).
EGRIFTA WRTM is not indicated for weight loss management.
EGRIFTA WRTM is not approved for use in clinical conditions other than the reduction of EVAF.
* The primary outcome for these trials was change from Week 0–26 in VAT by treatment group.
† An ≥8% decrease in VAT area was determined to be clinically significant and used to define responders a priori.
‡ Mean change (±SD) in fasting glucose levels between tesamorelin responders and non-responders: (Week 0-26: 1 ± 16 mg/dL vs. 5 ± 14 mg/dL [p=0.010]; Week 0-52: -1 ± 14 mg/dL vs. 8 ± 14 mg/dL [p<0.001]).
§ Mean change (±SD) in fasting insulin levels between tesamorelin responders and non-responders: (Week 0-26: -1.1 ± 25.2 µIU/mL vs. 5.7 ± 13.5 µIU/mL [p=0.011]; Week 0-52: -2.5 ± 19.1 µIU/mL vs. 4.9 ± 17.9 µIU/mL [p=0.002]).
¶ Mean change (±SD) in HbA1c levels between tesamorelin responders and non-responders: (Week 0-26: 0.1 ± 0.3% vs. 0.3 ± 0.4% [p<0.001]; Week 0-52: 0.0 ± 0.3 % vs. 0.2 ± 0.5 % [p=0.003]).
** Mean change (±SD) in HOMA-IR score between tesamorelin responders and non-responders: (Week 0-26: -0.4 ± 7.9 vs. 1.8 ± 4.3 [p=0.006]; Week 0-52: -0.7 ± 5.2 vs. 1.6 ± 5.5 [p<0.001]).
†† Mean change (±SD) in 2-hour glucose levels between tesamorelin responders and non-responders: (Week 0-26: -1 ± 34 mg/dL vs. 10 ± 44 mg/dL [p=0.009]; Week 0-52: -5 ± 37 mg/dL vs. 10 ± 31 mg/dL [p=0.006]).
‡‡ Mean change (±SD) in triglyceride levels between tesamorelin responders and non-responders: (Week 0-26: -0.6 ± 1.7 mmol/L vs. -0.1 ± 1.2 mmol/L [p=0.005]; Week 0-52: -0.8 ± 1.8 mmol/L vs. 0.0 ± 1.1 mmol/L [p=0.003]).
§§ Mean change (±SD) in adiponectin levels between tesamorelin responders and non-responders: (Week 0-26: 1.0 ± 3.0 µg/mL vs. -0.30 ± 1.8 µg/mL [p=0.011]; Week 0-52: 2.3 ± 3.2 µg/mL vs. 0.3 ± 1.6 µg/mL [p=0.008]).
* The safety of EGRIFTA WRTM (11.6 mg/vial formulation) has been established based on clinical trials conducted with EGRIFTA® (1 mg/vial formulation). Adverse events for the 1.28 mg dose (11.6 mg/vial formulation) of EGRIFTA WRTM are expected to be similar to those observed with the 2 mg dose (1 mg/vial formulation) of EGRIFTA®.
BMI = body mass index; CT = computed tomography; EVAF, excess visceral abdominal fat; FBG = fasting blood glucose; FDA = Food and Drug Administration; GH = growth hormone; HOMA-IR = homeostatic model assessment for insulin resistance; NDA = New Drug Application; PWH = people with HIV; VAT = visceral adipose tissue.
References:
Theratechnologies Inc. EGRIFTA WRTM (tesamorelin) for injection Prescribing Information. March, 2025.
Snyder SW. Regulatory Considerations for the Treatment of Lipodystrophy. Report of a Forum for Collaborative HIV Research Roundtable discussion. October 25, 2004; Washington DC.
Stanley TL, et al. Reduction in visceral adiposity is associated with an improved metabolic profile in HIV-infected patients receiving tesamorelin. Clin Infect Dis. 2012;54(11):1642-1651.
Let’s keep in touch
Enter your contact details to stay up to date with the latest developments from Theratechnologies.
IMPORTANT SAFETY INFORMATION ABOUT EGRIFTA WRTM (TESAMORELIN) FOR INJECTION
Indication
EGRIFTA WRTM is indicated for the reduction of excess abdominal fat in HIV-infected adult patients with lipodystrophy.
Limitations of Use:
The impact and safety of EGRIFTA WRTM on cardiovascular health has not been studied.
EGRIFTA WRTM is not indicated for weight loss management.
It is not known whether taking EGRIFTA WRTM helps improve compliance with anti-retroviral medications.
Contraindications:
Do not use EGRIFTA WRTM if patient:
Has a pituitary gland tumor, has had pituitary gland surgery, has other problems related to their pituitary gland, or has had radiation treatment to their head or a head injury.
Has active cancer.
Is allergic to tesamorelin or any of the ingredients in EGRIFTA WRTM.
Is pregnant or planning to become pregnant.
Warnings and Precautions
Increased risk of neoplasms: Preexisting malignancy should be inactive and its treatment complete prior to starting EGRIFTA WRTM. EGRIFTA WRTM should be discontinued if the patient has evidence of recurrent malignancy.
Elevated IGF-1: Regularly monitor IGF-1 levels in all patients during EGRIFTA WRTM therapy. Consider discontinuing in patients with persistent elevations (e.g., >3 SDS).
Fluid retention: May include edema, arthralgia, and carpal tunnel syndrome.
Glucose intolerance or diabetes mellitus: May develop with EGRIFTA WRTM treatment. Evaluate glucose status prior to and during therapy with EGRIFTA WRTM.
Hypersensitivity reactions: Advise patients to seek immediate medical attention if suspected.
Injection site reactions: Advise patients to rotate sites to different areas of the abdomen to decrease injection site reactions.
Increased mortality in patients with acute critical illness: Consider discontinuation in critically ill patients.
Drug Interactions
EGRIFTA WRTM had no significant impact on the pharmacokinetic profiles of simvastatin in healthy subjects.
Monitor patients for potential interactions when administering EGRIFTA WRTM in combination with other drugs known to be metabolized by CYP450 liver enzyme.
Patients on glucocorticoids may require dosage adjustment upon initiation of EGRIFTA WRTM.
Use in Specific Populations
Lactation: Mothers should not breastfeed if they receive EGRIFTA WRTM.
Pediatric use: Safety and effectiveness in pediatric patients have not been established.
Geriatric use: There is no information on the use of EGRIFTA WRTM in patients greater than 65 years of age.
Adverse Reactions
The most commonly reported adverse reactions include injection site reactions, arthralgia, pain in extremity, myalgia, and peripheral edema.
For more information about EGRIFTA WRTM, contact toll-free at 1-833-23THERA (1-833-238-4372). To report suspected adverse reactions, contact or the FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.